
The corneal stroma plays a critical role in LASIK, as it forms the structural foundation of the cornea and undergoes reshaping during the procedure to correct refractive errors.
Understanding its anatomy, physiology, and the biomechanical changes induced by LASIK is crucial for optimising patient outcomes and minimising risks.
Anatomy of the Corneal Stroma
The corneal stroma is the thickest layer of the cornea, contributing approximately 90% of its total thickness. Located between the Bowman’s layer and Descemet’s membrane, the stroma comprises a highly organised, collagen-rich extracellular matrix. This matrix includes type I collagen fibrils arranged in parallel lamellae, which are responsible for the cornea’s transparency and strength. Keratocytes, the primary cellular component of the stroma, maintain the collagen and glycosaminoglycan matrix, ensuring structural integrity.
Other key components include:
- Water content (approximately 78%): Essential for corneal clarity.
- Proteoglycans such as keratan sulphate and dermatan sulphate, which interact with collagen fibrils.
- Nerve fibres that provide sensory innervation to the cornea.
The unique arrangement and properties of the corneal stroma are what allow it to maintain its optical clarity while providing mechanical stability—a fine balance critical for vision and LASIK surgery.
Role of the Corneal Stroma During LASIK
LASIK, or laser-assisted in situ keratomileusis, reshapes the cornea to correct refractive errors like myopia, hyperopia, and astigmatism. The procedure involves creating a flap in the anterior cornea and ablating the stroma with an excimer laser to achieve the desired refractive correction. The corneal stroma is the key target layer for laser ablation, making its properties pivotal to the success of the surgery.
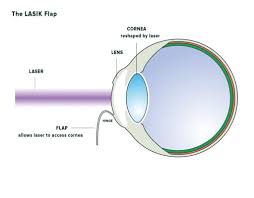
1. Creating the Corneal Flap
The first step in LASIK surgery involves creating a flap in the cornea using a microkeratome or femtosecond laser.
- The flap consists of the epithelium, Bowman’s layer, and the anterior portion of the stroma.
- The underlying deeper stromal bed is exposed for laser ablation.
The flap’s thickness is critical, as it determines the residual stromal bed thickness. A thin residual stromal bed increases the risk of post-LASIK complications, such as ectasia.
2. Stromal Ablation for Refractive Correction
The excimer laser is used to ablate the corneal stroma in a precise manner, altering its curvature to modify the cornea’s refractive power. The process involves:
- Targeting stromal tissue based on the patient’s refractive error.
- Myopia correction involves flattening the central cornea.
- Hyperopia correction steepens the periphery of the cornea.
- Astigmatism correction smooths irregularities in the stromal contour.
- Custom wavefront-guided ablation to address higher-order aberrations.
The stromal layer’s optical and biomechanical properties are directly affected by this reshaping, impacting the visual outcome and overall structural integrity.
Biomechanical Integrity of the Corneal Stroma
The corneal stroma’s strength and elasticity are critical to maintaining corneal shape after LASIK. However, laser ablation disrupts the stromal lamellae and reduces its biomechanical stability.
Factors Affecting Biomechanical Stability
1. Residual Stromal Bed Thickness (RSBT):
- Maintaining a minimum RSBT (usually 250 µm) is crucial for safety.
- Excessive ablation can weaken the cornea, leading to post-LASIK ectasia.
- Collagen Lamellae Alignment:
- The stromal lamellae’s orthogonal arrangement contributes to corneal stiffness.
- Disruption during ablation can lead to biomechanical weakening.
- Patient-Specific Variables:
- Pre-existing conditions like keratoconus or thin corneas increase the risk of complications.
- Biomechanical properties vary among individuals and should be assessed preoperatively.
Advances in Biomechanical Assessment
Modern LASIK procedures utilise advanced tools like corneal tomography and ocular response analysers to evaluate individual stromal properties. This preoperative assessment ensures customised treatments, reducing risks and improving outcomes.
Corneal Stroma and Post-LASIK Healing
The corneal stroma’s response to LASIK surgery involves a cascade of healing processes. These include:
- Stromal Wound Healing:
- Keratocytes migrate to the ablation site, synthesising new collagen and extracellular matrix.
- While partial restoration occurs, the newly synthesised collagen differs in alignment from the original lamellae, potentially affecting biomechanics.
- Remodelling of Keratocytes:
- Some keratocytes differentiate into fibroblasts or myofibroblasts, contributing to wound contraction and potential scarring.
- Transparency Maintenance:
- Proteoglycan interactions and water content regulation prevent haze formation, although some transient haze may occur during early healing stages.
Post-operative care often includes anti-inflammatory eye drops to control the healing response and minimise complications.
Complications Related to the Corneal Stroma
Despite advances in LASIK techniques, stromal alterations can lead to certain complications if not properly managed. Understanding the role of the stroma helps mitigate these risks.
1. Corneal Ectasia
Post-LASIK ectasia, a condition characterised by progressive corneal thinning and bulging, is associated with excessive stromal tissue removal or pre-existing biomechanical weakness. Preventative measures include:
- Rigorous preoperative screening for keratoconus or thin corneas.
- Adhering to safety margins for RSBT.
2. Dry Eye Syndrome
LASIK disrupts corneal nerves in the stroma, reducing tear production and causing post-LASIK dry eye syndrome. Most cases resolve within six months, but frequent artificial tear use may be necessary.
3. Regression of Refractive Error
Minor regression can occur due to stromal remodelling or epithelial thickening. Enhancement surgeries may address significant regression.
4. Residual Haze
Some patients may experience transient haze due to stromal wound healing and myofibroblast activity. Anti-inflammatory therapy typically resolves this issue.
Recent Developments in LASIK and the Corneal Stroma
Ongoing research aims to optimise LASIK outcomes by preserving or enhancing stromal integrity. Innovations include:
- Corneal Cross-Linking (CXL):
- Combining CXL with LASIK strengthens collagen cross-links in the stroma, reducing ectasia risks.
- Femtosecond Laser Technology:
- High-precision femtosecond lasers minimise stromal disruption, enabling thinner flaps and customised ablations.
- Topography-Guided LASIK:
- Utilises preoperative corneal maps to tailor stromal ablation, improving visual outcomes and reducing irregularities.
- Artificial Intelligence (AI):
- AI is being integrated into LASIK planning to predict outcomes and optimise stromal preservation.
Importance of the Corneal Stroma in Advancing LASIK Surgery
The corneal stroma remains the focal point of LASIK surgery, both as the layer undergoing reshaping and as a determinant of overall corneal stability. A thorough understanding of stromal properties allows eye surgeons to customise LASIK procedures for individual patients, balancing refractive correction with biomechanical safety.
With ongoing innovations and a focus on stromal preservation, LASIK has the potential to achieve even greater safety and efficacy. Continued research into the corneal stroma’s unique properties will undoubtedly shape the future of refractive surgery.
LASIK researchers, surgeons, and students alike can leverage this knowledge to improve patient care. By staying informed about the critical role of the corneal stroma in LASIK, the field can advance toward safer procedures and superior visual outcomes.