
Preoperative corneal thickness is key in determining LASIK suitability. A minimum of 500 microns is ideal to ensure safety and reduce complications.
The preoperative evaluation of corneal thickness is paramount in understanding how well the cornea will tolerate the surgical reshaping required during LASIK (Laser-Assisted in Situ Keratomileusis). This step ensures that sufficient corneal tissue remains post-surgery to maintain the structural integrity of the eye. Below, we will explore the key aspects of corneal thickness and its role in LASIK outcomes.
Why Corneal Thickness Matters for LASIK?
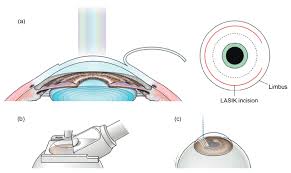
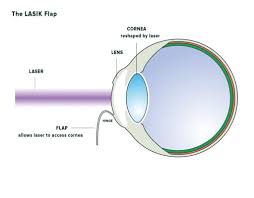
The success of LASIK relies heavily on precise alterations to the cornea to correct refractive errors like myopia, hyperopia, and astigmatism. However, reshaping the cornea involves removing tissue via an excimer laser. If the cornea is too thin to start with, it increases the risk of complications, such as ectasia (a condition where the cornea becomes weakened and bulges outward). Hence, measuring and assessing corneal thickness preoperatively is one of the primary steps to evaluating LASIK candidacy.
Corneal thickness, medically termed pachymetry, defines the health of the cornea and sets safety parameters for each LASIK procedure. The recommended minimum residual corneal thickness (after tissue removal) is typically 250-300 microns, which ensures the cornea remains stable after reshaping.
Standard Preoperative Measurements
1. Normal Corneal Thickness
The average thickness of a healthy human cornea is approximately 540 microns at its centre, with the peripheral regions slightly thicker. Patients with below-normal values may undergo additional testing to evaluate their LASIK eligibility, as the standard threshold of safety becomes harder to meet with thinner corneas.
2. Eligibility for LASIK
- Minimum thickness requirement: Most surgeons recommend avoiding LASIK if the corneal thickness is below 500 microns prior to surgery.
- Residual thickness safety threshold: Post-ablation, at least 250-300 microns of corneal stroma must remain intact to support corneal biomechanics and prevent instability.
The laser in LASIK removes approximately 12-15 microns of tissue per dioptre of correction, meaning the higher the patient’s refractive error, the more corneal thickness is required for successful surgery without compromising safety.
3. Diagnostic Tools for Measuring Corneal Thickness
To accurately assess corneal pachymetry, ophthalmologists use advanced diagnostic instruments such as:
- Ultrasound Pachymetry: A traditional method that uses ultrasound waves to measure corneal thickness.
- Optical Coherence Tomography (OCT): Offers high-resolution imaging of the corneal layers with precise thickness information.
- Scheimpflug Imaging (e.g., Pentacam): Provides a 3D corneal thickness profile, ensuring better mapping for irregularities and thin zones.
Factors Impacting Preoperative Corneal Thickness
1. Corneal Irregularities and Conditions
Certain conditions predispose the cornea to thinning, making LASIK a less suitable option:
- Keratoconus (progressive thinning and cone-shaped corneal deformity): Contraindicated for LASIK due to weak structural integrity.
- Pellucid Marginal Degeneration (PMD): Another contraindication due to peripheral corneal thinning.
- Post-Surgical Changes (e.g., previous corneal surgeries): These can reduce the central corneal thickness and affect subsequent procedures.
2. Refractive Error Severity
Patients with high myopia or astigmatism require more tissue ablation, demanding a thicker initial cornea to ensure sufficient residual tissue remains post-surgery.
3. Age and Demographics
Corneal thickness can experience subtle age-related changes. Younger individuals often have thicker corneas and are better suited for surgery. Ethnic variations may also influence baseline thickness, with studies showing slightly thinner corneas in certain populations.
Alternate Options for Thin Corneas
When corneal thickness is insufficient for LASIK, it doesn’t necessarily exclude the patient from refractive surgery. Other methods may be recommended:
- PRK (Photorefractive Keratectomy): Removes the epithelial layer without creating a flap, making it safer for thinner corneas.
- SMILE (Small Incision Lenticule Extraction): Uses less corneal tissue during correction and offers a viable alternative.
- ICL (Implantable Collamer Lens): Avoids reshaping the cornea altogether, instead implanting a lens in the eye to correct refractive errors.
Potential LASIK Complications Related to Corneal Thickness
Understanding preoperative corneal thickness helps mitigate surgical risks, but thin or improperly assessed corneas can result in the following complications:
1. Corneal Ectasia
This postoperative complication is characterised by a progressive thinning and bulging of the cornea and is most commonly linked to inadequate residual stromal thickness.
2. Irregular Astigmatism
Uneven tissue removal during LASIK can lead to visual distortions and irregular astigmatism, exacerbated by thinner corneas.
3. Reduced Corneal Integrity
A cornea with insufficient thickness may have compromised biomechanical strength, leading to visual instability or long-term changes in corneal shape.
How Surgeons Determine LASIK Suitability?
1. Individualised Surgery Planning
Modern LASIK procedures involve advanced customisation to tailor the surgical plan to the individual’s unique corneal anatomy. Surgeons carefully balance the patient’s refractive error with their corneal thickness to ensure precise and safe outcomes.
2. Optimising Ablation Profiles
By using advanced excimer laser technology, ablation depth is optimised, ensuring minimal tissue removal without compromising results. Additionally, wavefront-guided and topography-guided LASIK enhance safety for those with borderline-thick corneas.
3. Postoperative Follow-Up
Patients with thinner corneas may benefit from close postoperative monitoring to identify any early signs of complications like ectasia.
Final Thoughts – The Importance of Preoperative Corneal Thickness in LASIK
Preoperative corneal thickness plays a pivotal role in determining LASIK eligibility, safety, and post-surgery outcomes. With a minimum threshold of 500 microns, this metric allows surgeons to design a procedure that preserves corneal health and maximises visual improvements.
Surgeons must always approach LASIK candidates with precision diagnostics, detailed evaluations, and sound clinical judgment. By leveraging advanced imaging tools and planning techniques, ophthalmologists and surgeons can achieve successful outcomes while minimising risks.
For patients with borderline thickness or other contraindications—there are still plenty of refractive surgery alternatives to explore. Always consult an experienced ophthalmologist to assess your options comprehensively.