
Residual thickness after LASIK surgery is calculated by subtracting the tissue removed during ablation from the original thickness of the cornea, ensuring that the remaining tissue meets the safety threshold.
This calculation is crucial for the success of the procedure and the long-term health of the patient’s eyes.
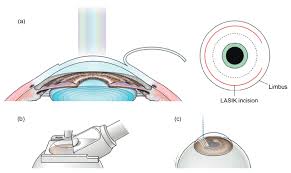
LASIK (Laser-Assisted in Situ Keratomileusis) is a common and highly effective refractive surgery designed to improve vision by reshaping the cornea. However, the procedure involves removing part of the corneal tissue, which can impact the structural integrity of the eye if not carefully managed. Residual thickness is one of the most important factors in determining whether a patient is a suitable candidate for LASIK and predicting the safety and success of the surgery.
To guide both patients and ophthalmologists, let’s explore the significance of residual corneal thickness, step-by-step calculations, and the parameters that influence it.
Why is Residual Thickness Important?
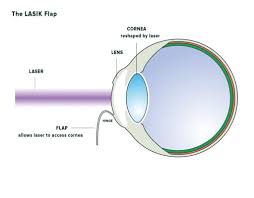
The cornea plays a key role in focusing light onto the retina, ensuring clear vision. During LASIK, the cornea is reshaped by removing precise layers of tissue. However, if too much tissue is removed, the structural stability of the cornea may be compromised, leading to complications like corneal ectasia—a condition that causes the cornea to bulge outward and result in distorted vision.
To avoid these complications, a sufficient amount of corneal tissue must remain after the procedure. The generally accepted safety threshold for residual stromal thickness is at least 250 microns. Beyond this number, surgeons also aim to preserve an additional margin to account for future stability and individual variations.
How to Calculate Residual Thickness After LASIK?
The calculation of residual corneal thickness involves several steps and relies on accurate preoperative measurements, the surgical technique used, and the specific parameters applied during laser ablation. Below is a systematic breakdown of the process.
1. Measure the Preoperative Corneal Thickness
The first step is to determine the cornea’s initial thickness (called the pachymetry value) using tools like a corneal pachymeter or optical coherence tomography (OCT). The average corneal thickness in a healthy individual typically ranges from 520 to 550 microns, but this can vary.
This value forms the foundation of the calculation. For example:
- Preoperative corneal thickness = 550 microns (example value)
2. Determine the LASIK Flap Thickness
During LASIK, a flap is created on the corneal surface, which is then lifted to perform the reshaping. This flap’s thickness is crucial to calculate the remaining tissue. While the thickness varies depending on the technology used (mechanical microkeratome vs femtosecond laser), it is often 110–120 microns for most procedures.
For this calculation:
- Estimated flap thickness = 120 microns (example value)
3. Calculate the Ablation Depth
The ablation depth refers to the amount of tissue removed from the corneal stroma during reshaping. This depth depends on the patient’s refractive error and the laser system’s ablation rate. A general rule of thumb is that approximately 12–14 microns of tissue is removed for every dioptre (D) of correction.
For instance:
- Correction needed for refractive error = -4.00 D
- Estimated ablation depth = 4 x 14 microns = 56 microns
4. Subtract the Flap Thickness and Ablation Depth
Subtract the laser-induced ablation depth and flap thickness from the preoperative corneal thickness. This gives the residual thickness after LASIK. Using the example values:
- Preoperative corneal thickness = 550 microns
- Flap thickness = 120 microns
- Ablation depth = 56 microns
Residual thickness = 550 – 120 – 56 = 374 microns
This final calculation indicates that the residual stromal thickness is 374 microns, which is above the safety threshold of 250 microns. Hence, the procedure is safe for this patient.
5. Confirm with Safety Margins
While 250 microns is widely accepted as the minimum safe thickness, most surgeons prefer a margin of at least 300 microns to account for long-term corneal stability.
Formula for Quick Reference
Here’s a simplified formula for calculating residual thickness:
Residual Thickness = Preoperative Corneal Thickness – Flap Thickness – (Dioptres x Ablation Rate)
Where:
- Flap thickness is typically 110–120 microns
- The ablation rate is approximately 12–14 microns/dioptre
Key Factors That Influence Residual Thickness
The exact calculation of residual thickness depends on several variables. Below are some critical factors that influence the final result:
1. Preoperative Measurements
Accurate pachymetry readings are essential for precise calculations. Advanced imaging tools like optical coherence tomography (OCT) provide highly detailed analyses of corneal thickness and are increasingly used by ophthalmologists.
2. Depth of the Flap
The technique used to create the LASIK flap has a significant impact on thickness. Modern femtosecond laser technology allows for greater precision, creating thinner and more consistent flaps compared to older microkeratomes.
3. Degree of Refractive Error
Higher refractive errors require greater ablation depths, which in turn reduces the residual thickness. Patients with extreme myopia, in particular, may not have enough corneal tissue to safely undergo LASIK. For these patients, alternative procedures like PRK (Photorefractive Keratectomy) or SMILE (Small Incision Lenticule Extraction) may be recommended.
4. Laser System and Technology
The efficiency and precision of the laser system used can also influence tissue removal. Advanced excimer lasers are designed to remove tissue with greater accuracy while minimising collateral damage.
5. Individual Variations
Biological factors such as corneal elasticity, hydration levels, and pre-existing conditions (e.g., keratoconus) can impact the cornea’s response to the procedure and the overall residual thickness.
Tools Used for Calculating Residual Thickness
Precision is everything in eye surgery, and advanced technology makes the process safer and more reliable. The following tools are commonly used for measurements and calculations:
- Pachymeters for measuring corneal thickness.
- Topographers and Tomographers for mapping the curvature and thickness of the cornea.
- Excimer and Femtosecond Lasers used during the LASIK procedure, equipped with integrated measurement systems.
Alternative Procedures for Thin Corneas
If a patient’s calculated residual thickness after LASIK falls below the safety margin, other refractive surgeries may be considered, such as:
- PRK (Photorefractive Keratectomy): This technique removes the corneal epithelium (no flap creation) and requires less corneal depth.
- SMILE (Small Incision Lenticule Extraction): A flap-free, minimally invasive approach suitable for some patients.
- Phakic IOLs: Implantable lenses that correct refractive error without reshaping the cornea.
Wrapping Up
Calculating residual corneal thickness after LASIK is a crucial step in ensuring the safety and long-term success of the procedure. By combining precise preoperative measurements, an understanding of refractive corrections, and advanced technology, ophthalmologists can achieve remarkable outcomes for their patients.
If you’re a LASIK patient, ensure your surgeon discusses residual thickness as part of the pre-surgical evaluation. For ophthalmologists and eye-care professionals, staying informed about the latest tools and techniques is key to offering the best care.
Prioritising safety and precision ensures a clear, distortion-free future for those opting for this life-changing procedure.