Table of Contents
ToggleWhether blade-free LASIK or frame-to-second LASIK, all forms of LASIK surgery are 100% detectable. All can be viewed by an eye doctor using a slit lamp or microscope and are detectable. Even if the issue is not widespread, a slit lamp cannot pick it up. But Lasik can be quickly recognized.
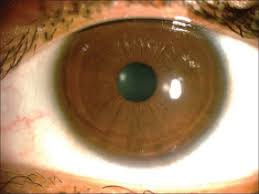
So, to put it simply, it is possible to identify Lasik surgery on the eyes by looking at the corneal surface. The Lasik technique involves two phases. The Bowman’s or corneal epithelial layer is sliced during the first phase to generate the flap. Both blades and lasers can be used in this technique. The borders of the corneal flap, generated on the top of the cornea, can serve as a visual cue that Lasik surgery has been done. Even years after Lasik surgery, this is still easily detectable by an eye doctor under a slit light or microscope.
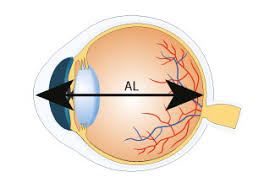
The presence or absence of Lasik surgery in the eyes can be easily determined by eye specialists using cutting-edge diagnostic tools like Pentacam. Following Lasik, the cornea’s overall thickness is decreased, and the shape of the eyes is changed. With an advanced diagnostic system assessment, experts can quickly discover such modifications.
Symptoms of Lasik eye surgery
- Your eye may itch, feel gritty, burn, and be watery just after surgery.
- Your vision will likely be hazy. In most cases, you won’t experience discomfort, and your vision will recover quickly.
- You could be given medicines or eye drops to help you feel better for a few hours after the procedure.
Although LASIK surgery has permanent results, its benefits can deteriorate over time. For most patients, LASIK will have long-lasting benefits.
Anatomical alterations to the eye or eyes will require an augmentation operation in about 10-12% of individuals nationwide.
LASIK Testing
Testing is essential in the LASIK assessment, and proper testing is required for a person to be effectively screened.
Contrast Sensitivity Evaluation
Beyond the Snellen chart, some clinicians may perform contrast sensitivity tests to evaluate better the patient’s functional vision (a high contrast chart). Present-day testing includes, for example, the Mars Letter Contrast Sensitivity Test and the Hamilton-Veale Contrast Sensitivity Test.
Pupil Evaluation
Pupil size evaluation will allow for more informed consent, particularly in the dark. Special instruments, including an infrared pupilometer, can accurately measure pupil size. Patients with bigger pupil diameters may experience glare and halos following LASIK surgery. On the other hand, the relationship between pupil size and surgical symptoms is still being contested.
Dry Eye Examination
Patients with pre-existing ocular dryness who have LASIK surgery will be at an increased danger of post-operative dryness. If eye dryness is identified, therapy is initiated immediately. Tears break up time assesses the tear film’s quality. If the results are incorrect, lid hygiene and additional blepharitis therapies are started. Schirmer testing determines the quantity of tear film. If the results are abnormal, therapies such as tear substitutes, punctual plugs, nutritional supplements (fish oil or flax), cyclosporine, and lifitegrast are initiated. Patients will undergo ongoing monitoring and re-evaluation until their dryness improves before LASIK can be done. Tear osmolarity testing, for example, is increasingly popular among refractive surgery patients. Non-invasive tear break-up time (NIBUT), lipid layer assessment at the slit-lamp biomicroscope using specular reflection and a qualitative grading scale, and meibography, which is imaging with photography (such as the Oculus Keratography 5M), are additional tests for tear film stability.
Topography, Tomography, and Corneal Biomechanics
Biomechanics of the cornea, topography, and tomography corneal topography, also known as computerized video keratography, has unquestionably contributed to the development of refractive surgery. The Greek words topos (place) and graphein (to write) are the origins of the term topography. Corneal topography is a front or anterior corneal surface imaging technique, even though topography has traditionally been associated with studying geographical elements like the Earth’s surface shape and features. The Greek words Tomos (a cut or section) and graphein (to write) are the origins of the term tomography.
A mathematical method for calculating a solid organ’s 3-D structure is called tomography. As a result, thickness mapping and diagnostic characterization of the cornea’s front and back surfaces ought to be referred to as corneal tomography. Horizontal slit scanning, rotational Scheimpflug imaging, arc scanning with high-frequency ultrasound, and anterior segment optical coherence tomography are among the tomography technologies supported by various commercial instruments.
The corneal characterization should go beyond single-point central thickness and front surface curvature to increase the sensitivity and specificity of screening protocols for candidates for refractive surgery. A tomographic method is necessary. To reconstruct corneal architecture in three dimensions, tomography combines complete tachymetric data with elevations of the anterior and posterior corneas. It is challenging to interpret such a large amount of data.
Refractive surgeons should be aware that the detection of mild or subclinical forms of ecstatic diseases like keratoconus and pellucid marginal degeneration should not be the sole objective of screening candidates for refractive surgery for ectasia risk; it ought to also take into account how susceptible a cornea that is relatively normal to biomechanical failure.
Wavefront Evaluation
Wavefront testing is utilized to find higher-order abnormalities that could impair vision. Patients with considerably higher-order aberration cannot be treated with standard LASIK techniques, which may leave them with unfavourable visual side effects after surgery. Wavefront-controlled LASIK may be superior to lower higher-order aberrations and improve the patient’s vision.
Conclusion
The initial Excimer laser method is typically referred to as PRK. The outcomes of the more recent PRK modifications and the application of tissue healing modulators have significantly improved. The more recent methods are called ASA or advanced surface ablation. In contrast to LASIK, neither PRK nor ASA involves the creation of a flap; instead, only excimer laser surface ablation is performed after the corneal epithelium has been removed through various methods. The pain following ASA is only mild to moderate. In ASA, corneal haze and regression are virtually non-existent, making them the most challenging to detect later.